
Over 50% of those with clinical level mental health risks do not seek help. The major reasons of thinking that it won’t help or not knowing what kind of help to seek, shine a light on the lack of treatment efficacy and research challenge in mental health.
According to some estimates, only 1 in 5 people diagnosed with major depression in high income countries, and 1 in 27 in low/middle income countries, receive minimally adequate treatment for their symptoms and distress [1]. Other data from the US indicates that, between 2008 and 2014, approximately 30% people with major depression reported needing but not receiving mental health treatment [2]. Similar treatment gaps are found for other disorders [3-6]. Understanding the reasons behind these statistics, and therefore the existing barriers to care seeking, is essential to ensure that people suffering from mental health disorders receive the required care and support, and also to guide policy decisions relating to care provision and promotion.
In the Global Mind project (which currently encompasses 100,000+ MHQ responses) we ask respondents who are not currently seeking help for a mental health disorder why this is the case. Their answers help illuminate the perceived barriers to care seeking that people commonly experience.
The majority with clinical mental health challenges do not seek help.
Across the 10 English-speaking populations that we currently study, 58% of respondents who had MHQ scores below 0 – indicating that they were clinical or at risk for a disorder – reported not seeking help for their mental health challenges. In the United States the number was 45% and in the UK it was 50%. In Australia and Canada the number was 45% and 47% respectively, meaning 55% and 53% did seek help. In contrast in South Africa, Singapore, Nigeria and India those not seeking help ranged from 61% to 81%.

Conversely, it is interesting to note that across these 10 countries, 16% of those without clinical level mental health challenges i.e. in the categories of enduring to thriving on the MHQ scale, nonetheless sought help for sub clinical challenges. In the United States this percentage was 21% and in the United Kingdom it was 17%.
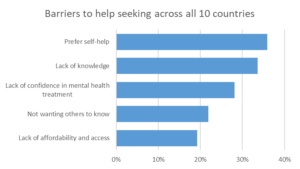
Lack of knowledge and confidence in treatment are key deterrents to help seeking.
Digging into the perceived barriers to care seeking across the data we find that, overall, respondents with clinical or at risk MHQ scores who did not seek help for a mental health problem reported that the primary reason for not doing so was a preference for self-help (36%). This suggests that they preferred to manage their challenges on their own or did not think they needed mental health treatment or therapies. Other major barriers included a lack of knowledge of what kind of help to seek or where to get it (34%) and a lack of confidence in mental health treatments (28%), which was largely due to respondents feeling that it wouldn’t help (19%) or because they were fearful of being forced to take a medication or being committed (13%). 22% of respondents were deterred from help seeking due to fear of not wanting people to know, potentially due to stigma, and 19% were deterred by lack of affordability and access.
However, looking across different countries, we found that this ranking of barriers differed. In the United States lack of confidence in mental health treatments topped the list at 37%, followed by a lack of knowledge (34%). These also topped the list in the United Kingdom at 32% for both. In Singapore, there was a preference for handling difficulties without treatment (30%) while both India and Singapore had the highest percentage reporting that they had no need for any mental health services (20%), despite reporting clinical/at risk MHQ scores. In the United States lack of affordability was an obstacle to getting help for 25% of people but was not a significant issue in the United Kingdom (less than 5%) where healthcare is nationalized.
Getting to solutions
The perceived barriers to care seeking are therefore multiple and differ across countries. However, one common theme that stood out across several countries is that many people struggled to know which type of help they should be seeking and/or had low confidence in the efficacy and delivery of available treatments. Although stigma and not wanting others to know was still a sizable barrier for many, the data largely points to the need for greater clarity in the mental health space to help individuals understand their specific challenges and direct them to the right resources.
The core challenge, however, is which resources? Most currently available medications and therapies tend to be effective only for a third of patients, and only partially so, introducing a great deal of trial and error [7]. Furthermore, as shown in the 2020 Mental State of the World Report, a greater number of psychiatrists per 100,000, while closely correlated to the fraction who seek help for clinical level challenges, does not ultimately have any bearing on clinical burden [8]. To make progress therefore requires addressing this root challenge from a research perspective. New approaches are required.
see related posts How True are DSM Disorder Classifications to Real Life Symptom Profiles and From Brain to Behavior: The Search for Biomarkers
Data from the Global Mind project is freely available for download by researchers for non-commercial purposes – you can request access here.
References:
[1] Thornicroft G, Chatterji S, Evans-Lacko S, et al. Undertreatment of people with major depressive disorder in 21 countries. Br J Psychiatry. 2017;210(2):119-124. doi:10.1192/bjp.bp.116.188078
[2] Chekroud AM, Foster D, Zheutlin AB, et al. Predicting Barriers to Treatment for Depression in a U.S. National Sample: A Cross-Sectional, Proof-of-Concept Study. Psychiatr Serv. 2018;69(8):927-934. doi:10.1176/appi.ps.201800094
[3] Bussing R, Zima BT, Gary FA, Garvan CW. Barriers to detection, help-seeking, and service use for children with ADHD symptoms. J Behav Health Serv Res. 2003 Apr-Jun;30(2):176-89. doi: 10.1007/BF02289806.
[4] Kantor V, Knefel M, Lueger-Schuster B. Perceived barriers and facilitators of mental health service utilization in adult trauma survivors: A systematic review. Clin Psychol Rev. 2017 Mar;52:52-68. doi: 10.1016/j.cpr.2016.12.001.
[5] Hart LM, Granillo MT, Jorm AF, Paxton SJ. Unmet need for treatment in the eating disorders: a systematic review of eating disorder specific treatment seeking among community cases. Clin Psychol Rev. 2011 Jul;31(5):727-35. doi: 10.1016/j.cpr.2011.03.004
[6] Kessler RC, Demler O, Frank RG, Olfson M, Pincus HA, Walters EE, Wang P, Wells KB, Zaslavsky AM. Prevalence and treatment of mental disorders, 1990 to 2003. N Engl J Med. 2005 Jun 16;352(24):2515-23. doi: 10.1056/NEJMsa043266.
[7] Cuijpers P, Christensen H. Are personalised treatments of adult depression finally within reach? Epidemiol Psychiatr Sci. 2017 Feb;26(1):40-42. doi: 10.1017/S204579601600007X.
[8] Newson JJ, Pastukh V, Sukhoi O, Taylor J and Thiagarajan TC, Mental State of the World 2020, Mental Health Million project, Sapien Labs, March 2021